Prepared by:
Emmanuel Timothy THWOL
PhD candidate, University of Juba
-
Executive summary
Kala-azar is endemic in this country especially at Upper Nile state. From last couple of months, there were unusual high number of cases treated in Malakal Teaching Hospital; primarily defined by the attending clinician as an outbreak. So, this reporter started investigating it with objectives of (i). Understanding the epidemiology of the suspected outbreak for immediate response and (ii) planning to minimize future risk of such outbreaks.
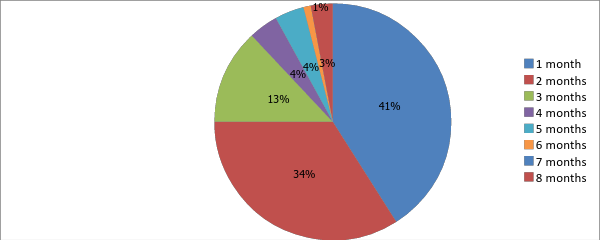
This investigator has to depend on hospital records only. According to the records, 50% of total cases (n=164) are from Malakal county, 25% from Baliet and 20% from Fashoda county. The outbreak seemed started from August and then sharply rose on September and October especially in Malakal County. Two-third of total cases is below 15 years age group: 34% under 5 years and 32% “5 to <15” year’s age group; uncommon in ≥35 years age (10% only). Most of the cases were malnourished (under-nutrition); about 14% (23) of total cases died mainly due to severe anaemia. Though it is not clear in the hospital records yet it is understood that Kala-azar patients are coming to the hospital late: 41% after one month of onset, 34% after 2 months and 13% after three months.
As the outbreak is still in upward trend and mainly in Malakal county among <15 years old children, an immediate outbreak response is critical. It includes: (i) uninterrupted supply of medicine for Kala-azar management (ii) equipping peripheral primary health care facility staffs especially in Makal county with knowledge and logistics for rapid diagnosis and referral and also (iii) establishing a community network for Kala-azar awareness, case identification and immediate referral in addition to Providing nets to the high risk community also important.
-
Introduction and background information
Kala-azar in this region occurs in 2 foci and is caused by L. donovani. In the one focus (Upper Nile, Jonglei, and Unity states), Phlebotomus orientalis is the vector. Epidemiologic modelling of data from Upper Nile state estimated that those who visited healthcare facilities from October 1998 through May 2002 represented only 55% of cases and that 91% of kala-azar deaths were undetected. Health coverage is so minimal that some patients must walk for several days to access even the most basic healthcare services. So, the cases detected at the Malakal Teaching Hospital in 2013 outbreak and number of known deaths might be tip of the iceberg especially in this rainy season of this highly inaccessible state.
-
Objective of the investigation
-
General objective
-
-
Conduct of an epidemiological investigation, situation analysis of the Kala-Azar outbreak and identifying the risks factors in the State in Upper Nile Sate.
-
Specific objectives
-
Understand the epidemiology (pick time, most affected place and person) of current Kala-azar outbreak in Upper Nile and response accordingly
-
Provide technical guidance to the State Ministry of Health (SMOH) and the relevant institutions on the magnetite of the outbreak
-
Future plan to minimize risk of Kala-azar outbreaks in Upper Nile state
-
Methodologies used in data collection
The study established an outbreak hypothesis and verifies all possibilities of Kala-azar occurrence through analysing all hazard factors and options, conducting assessment exercise in Malakal Teaching Hospital (MTH) , in addition filed visits to Health Facilities, Market place and residential areas were carried out to create clear scenario, accordingly the following details methods where conducted ;
-
Health facility visits and collection of epidemiological data
-
Community visits and assessment of environmental conditions
-
Key informant interview of key SMOH officials, stakeholders, community members and leaders
-
Collection of relevant samples for testing
-
Limitation of this investigating exercise
This investigation was conducted based on hospital record which is inadequate, not unique and not much specific to prepare a complete report. Even after cleaning data obtained from the hospital records, this investigator has to compromise with the quality of information/data and its analysis.
-
Epidemiology of the Kala Azar outbreak
-
Place
-
Kala-azar cases of Upper Nile outbreaks are mainly from 4 counties and also huge number (69) from a neighboring county, Pigi of Jonglei state. In Upper Nile state (n=164) about half of the cases are from Malakal (86), one fourth from Baliet (40), one fifth from Fashioda (32) and few (6) from Akoka county. Traditionally houses in these areas are made of soil without windows and most of these areas are bushy.
Map: Kala-azar case distribution by counties

|
About ²/3rd of total cases (n=164) are below 15 years old:34% from under 5 years age group and 32% from “5 to <15 years” group. Only 10% are from ≥ 35 years age group. Two third of total cases are male and remaining female; None pregnant. Almost all the adult patients (97%) were in <93% of “weight for height” range and none of the children with >18.2 BMI |
||||||
|
Weight for height % → |
<25% |
25 to <50% |
50 to <75% |
75 to <93% |
≥93% |
|
|
Kala-azar patients in % → |
38% |
0% |
30% |
30% |
2% |
|
-
Time Chart 2: Kala-azar cases by month of onset
|
There were 2 to 11 cases in each month from January to July 2013; seemed normal as the disease is endemic in this state. But there was a sharp rise in September and pick in October especially in Malakal (28 & 36 cases respectively).
|
-
Complication Chart 3: Status of anaemia (Hb gm/dl) in Kala-azar patients
|
About three fourth of total cases got moderate to severe anaemia as mentioned below (per dl)-
|
About 2% of the cases got
Hepatic failure
4.5. Case fatality rate
About 14% of the total detected cases (23 out of 164 cases) died; 20 of them due to severe anaemia, 1 due to anaemia with jaundice and 2 due to hepatic failure.
-
Discussion
It is assumed that about half of total Kala-azar cases are not seeking medical care from the hospital and about 90% of total death cases remained undetected. As all the cases are from neighbouring counties of Malakal Teaching Hospital, so there might be many more Kala-azar patients especially in the remote communities and significant number of those cases are dying home without proper medical care.
Two third of total cases are children and significant (34%) percentage are under 5 years age group; indicates lack of awareness about Kala-azar among parents to protect their children from sand fly bites.
Kala-azar patients especially from the distant places coming late (1 to 8 months after onset) for hospital care that indicates inadequate or absent social awareness program in Upper Nile state as well as poor screening facility at the primary health care facilities. The outbreak is at the pick in October and may continue unless community level intervention given.
-
Conclusion
Some shortage of drugs to manage Kala-azar patients in Malakal Teaching Hospital noticed. Interventions to save Kala-azar patients means saving children of Upper Nile as two thirds are under 15 years age.
8.Challenges
-
Inaccessibility of some areas (HFs) for an aim of getting broader picture, information gathering and evaluation of preparedness level at PHCUs due to lack of mobility means.
-
Inadequate multi-sector representation in the State.
-
Cross-border movements heighten the risk of communicable diseases
9.Lessons learned
-
Necessity for SMOH staff capacity building, surveillance system reform and emergency stockpiles preposition at State, County level is highly due to remoteness of health facilities and inaccessibility of roads.
-
Potentially need to extend support to counties hospitals to equip to response to any reported case.
-
Strengthening an area of sample collection ,shipment and examination
10. Recommendations
10.1. For immediate response:
-
Ensure uninterrupted supply of medicine for Kala-azar management at Malakal Teaching Hospital
-
Equip peripheral primary health care facility staffs especially in Malakla County with knowledge and logistics for rapid diagnosis and referral. Supplying nets for high risk community also critical
-
Provision of supplies: The provision of supplies required for outbreaks response activities; supplies should available in state or county.
-
Human resource development and training: Service quality in HFs should be maintained and improved by counting refresher trainings.
10.2. For late response: Establish a community network for Kala-azar awareness, case identification and immediate referral. A comprehensive plan for community level AFP surveillance, EmOC awareness and “Kala-azar awareness-identification-referral” system might be developed with the support of local partners.
References
-
SMOH IDSR /HIMS data base 2013
-
WHO Malak Sub office weekly bulletins (2013 )
-
WHO Malakal sub office Kalzar’s outbreak line -listing (2013)
-
WHO South Sudan emergency Response. Situation report epidemiological weeks #(13-43)
-
WHO-South Sudan Emergency response situation report Wpi Wks #1(3-452013).
Newer articles:
- UNITING THE DIASPORA FOR PEACE IN SOUTH SUDAN: BUILDING TRUST AND DOING GOOD - 02/08/2015 15:48
- A DOSSIER FOR TRUTH AND TRANSPARENCY SALVA KIIR MAYARDIIT’S LEADERSHIP-REGIME CHANGE AN IMMEDIATE PRIORITY - 31/07/2015 15:03
- South Sudan women - A Voice in the Wilderness of South Sudan - 26/07/2015 18:17
- Twic East Community of South Sudan-USA Press Release Event summary Report of July 4, 2015 in Syracuse, New York [The Empire State] - 26/07/2015 12:59
- Countering lawlessness in South Sudan - 20/07/2015 23:09
Older news items
- Academic Article Prevalence of Diarrhea and Malaria among Under Five Years Children in Rubkona IDPs - 17/07/2015 10:03
- A PAPER ON HEALTH SYSTEM MANAGEMENT; IT’S IMPACT UPON HEALTH INDICATORS PERFORMANCE A CASE OF UPPER NILE STATE, SOUTH SUDAN - 16/07/2015 18:49
- Conference Invitation : Achieving a sustainable peace in South Sudan, a community perspective - 16/07/2015 18:43
- Is Collo Lulled into a false Sense of Security? - 13/07/2015 10:23
- Thon Mangok hung up himself - 10/07/2015 13:52
Latest news items (all categories):
- Beyond The Tribal & Regional Lines: A Call for South Sudan's National Unity - 04/10/2025 21:17
- Frontmen for Businesses Linked to Sudan’s Rapid Support Forces Identified in the UAE - 04/10/2025 21:08
- South Sudan opposition leader Machar claims immunity in treason trial - 04/10/2025 14:39
- Death of a rainmaker: When drought means murder in South Sudan - 04/10/2025 14:33
- Great Hunger: South Sudan is at Tipping Point - 04/10/2025 14:27
Random articles (all categories):
- EAC Speakers want their association recognised in the region - 14/11/2022 00:02
- Minister Awut Deng: A New Iron Lady on a fake war on corruption - 01/12/2008 17:02
- The Fulfilled Drama of South Sudan Benydit and Guandit Not Bandit - Sudan Tribune - 27/03/2012 09:15
- ApTech installs 106 automatic drinking water dispensers in South Sudan - 12/11/2021 03:22
- Youth Should Stay Away From Political Uncles - 14/10/2019 17:51
Popular articles:
- The Final Communique of SPLM-DC Third Session of the National Council - 29/03/2011 01:00 - Read 80899 times
- Roles and Definition of Political Parties - 29/04/2011 01:00 - Read 63357 times
- Agriculture in Southern Sudan: Challenges and Investment Opportunities - 06/10/2010 01:45 - Read 47205 times
- Fashoda Youth Forum Rehabilitation of Drainage Culverts in Malakal town Report - 07/08/2008 16:22 - Read 34684 times
- Creation and establishment of the Local Government Councils ( Counties ) (2) - 28/09/2011 01:00 - Read 30389 times